- A
- A
- A

ADOPT AN INDEPENDENT LIVING APPROACH RATHER THAN MEDICAL MODEL OF LTC SERVICES.
The traditional model of long term care services emphasizes a medical approach to meeting needs, often involving unnecessary high cost professionals. The independent living (IL) approach to long term care services vests control of services in the consumer rather than the professional. Many of the services that are widely perceived as “medical” are simply a part of daily life to a person with disabilities. The independent living paradigm supports an integrated life in the community, with personal care workers providing needed assistance in tasks ranging from dressing and bathing to managing breathing devices, feeding tubes and catheters. Tasks that hospitals routinely train family members to perform can also be done in a home setting by other laypersons under the direction of the individual or their family member.
THE PARADIGM AT A GLANCE
DIMENSION MEDICAL MODEL (“Traditional”) INDEPENDENT LIVING MODEL
The table below conveys the contrast between the medical model and the independent living model. The fundamental difference between the two models is the contrasting perspectives of people with disabilities versus professionals on the practical realities of living with disabilities. The IL approach is hailed by people with disabilities because it not only produces higher consumer satisfaction, but it is more cost-effective than the traditional medical model. The medical model over-relies on expensive medical professionals and a paternalistic approach to service delivery. Thus, the dominant traditional system is insufficient to meet the needs of the consumers and is more costly to NYS. CDR urges NYS to shift toward an independent living approach by placing control over services with the consumer and reducing dependence on costly professionals.
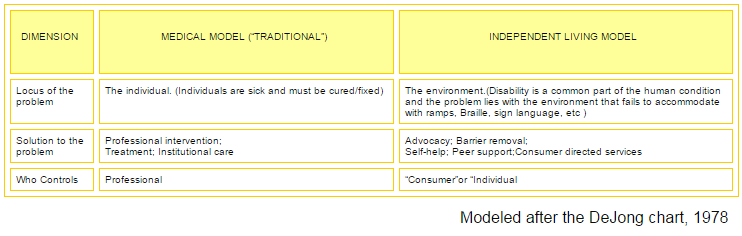
As the table conveys, the IL model views the problem as caused by the environment, not the individual. For example, the problem is not that a wheelchair user cannot walk; it is that a ramp is not provided for access to the building. The problem is not that a deaf person cannot hear; it is that sign communication is not available. It removes the blame from the person and the disability (which is non-controllable) and places the responsibility on society (which is controllable). A disability becomes limiting only in the context of an environment that does not accommodate the disability. When the barriers are removed and supports are provided, the disability becomes a manageable part of a full lifestyle.
BENEFITS OF INDEPENDENT LIVING
The IL approach promotes advocacy, barrier removal, self-help, peer support, and consumer directed services. These concepts empower the individual. This approach results in a distinctly different experience than a person has living under the traditional medical model, which focuses on trying to fix the broken person. Advocacy involves both systems advocacy to affect policy reform and self-advocacy to ensure individuals can attain the services they need. Because disabilities vary drastically, barrier removal directly addresses any obstacles to a productive community-based life for each individual. A systemic approach to barrier removal is also a necessary component to IL because it impacts everyone with a disability as opposed to individualized problem solving—which mimics the medical model approach of treating the broken person. Self-help and peer support are essential to the IL model because they embody the concept of independence within the context of a positive and shared disability identity.
Individuals with disabilities offer support, advice, and resources to other people with disabilities so they can live free from agency and institutional controls. People with disabilities receive training on independent living and learn skills which allow them to reduce their reliance on state and federal assistance programs. Finally, consumer directed services allow individuals to receive the services (medical and nonmedical) they require in order to live independently. A consumer directed approach removes the controls from the traditional agency and positions people with disabilities to be in charge of their services and supports. [The concept of consumer directed services is explained further in Vol. 4 of Reforming Long Term Care Services in New York State.]
Independent Living Centers (ILCs) promote the ideals espoused by the IL model. ILCs are run by people with disabilities for people with disabilities. According to a report produced by the Center for State Health Policy (CSHP),
“Centers for Independent Living continue to demonstrate their value in assisting individuals with disabilities of all ages to gain needed skills and obtain needed supports to live independently in integrated community settings…All services benefit both the individual receiving services and all levels of government. Individuals with disabilities have richer lives through the empowerment of freedom and independence. Government not only supports what individuals need and want, but it uses fewer resources to achieve those goals” (Independent Living Centers: Experienced Local Partners for Medicaid Home and Community-Based Services. Center for State Health Policy, Auerbach and Claypool, June 2008).
There are currently 34 members of the New York Association of Independent Living (NYAIL) across the state, which support the IL model.
DEMEDICALIZATION
What may be deemed a “medical” need by the general public is simply a part of daily life for people with disabilities. For example, catheterizing is no more a medical need to be performed by a registered nurse to a person with disabilities than an insulin shot is to a person with diabetes. However, outside the disability community, this need is classified as a medical need and therefore requires a medically licensed professional to perform the task. With this fundamentally medical model approach to long term care comes the added costs of medical service delivery and the disempowerment of the individual with disabilities.
In the medical paradigm, the person is a “patient in need of care.” The medical model does not look at the individual beyond their disability, but rather looks at the disability and determines how to “fix” it. This approach reinforces the institutional bias because, under the traditional approach, the more significant the disability, the more likely the perceived “fix” is isolation and sedation in a facility.
DIGNITY OF RISK
The IL model is about the freedom to take charge of one’s life and make personal choices. People with disabilities do not need to have their hands held to go through life. They do not want to be a part of a system that is patronizing and regards people as though they are incapable of making decisions or should be protected from the consequences of their decisions in ways that others are not. CSHP notes, “Advocates call for what most of us take for granted: the opportunity to assert the right to make informed decisions and to accept responsibility for any risk that is associated with those individual life decisions” (Advancing Medicaid HCBS Policy: From Capped Consumer to Consumer-Directed, Center for State Health Policy, Acosta and Hendrickson, March 2008). People with disabilities want the dignity of risk—including the option to fail.
There is a level of intrusion by service providers in the traditional agency model that does not exist in the consumer directed IL approach. Investigating and reporting requirements by agencies produce intrusive actions. For example, smoking involves risks to one’s health. Nondisabled people are free to take that risk; however, people with disabilities under an agency’s control have agency staff reporting on their personal choice of smoking because the agency interprets the act of smoking as a violation of their health care plan. The issue is not whether smoking is a health risk; the issue is that people with disabilities are viewed as unable to take the risk and make the choice for themselves.
This concept of risk directly correlates to administration and quality of services. People with disabilities want the freedom to direct their own care without the intervention of social workers and medical professionals. No one knows how to better manage their services than people with disabilities themselves. They are the experts and therefore they are the best evaluators of quality assurance.
ESSENTIAL COMPONENTS OF IL
The independent living model affords people with disabilities the dignity to take risks and direct their services in the community. In order to effectively adopt an independent living model, the focus of reform should be on the three essential community support services: (1) physical/cognitive support services; (2) accessible, affordable, integrated housing; and (3) transportation.
- Support Services: NYS must recognize the support services that encompass a variety of assistive programs beyond case management, including but not limited to, independent living skills training, assistive technology, environmental modifications, and personal care.
- Housing: Reforming long term care services to reflect an independent living approach cannot be achieved without a comprehensive housing plan to address the need for accessible, affordable, integrated housing. [The issue of housing will be explored in detail in Vol. 7 of Reforming Long Term Care Services in New York State.]
- Transportation: Transportation is an essential component to living an integrated lifestyle; however, transportation is not readily available for all individuals in NYS. Public transportation does not adequately accommodate people in rural communities, which comprise a significant portion of the state. Even in those communities where public transportation exists, for people with disabilities, daily challenges remain. With limited access to transportation, people with disabilities are confined to their homes–essentially creating a nursing home of one. NYS needs to increase community transit options.
CONCLUSION
The IL approach reflects the trend in long term care services toward a more consumer directed system. This important trend also serves as a noteworthy predictor of the needs of future long term care service users, aging baby boomers. No longer will people accept being treated as passive patients, but rather they will demand an active role in their long term care services—specifically directing who, when, where and how services will be administered.
LEGAL MILESTONES IN DISABILITY RIGHTS:
- 1964 Civil Rights Act (Prohibits discrimination on the basis of race, religion, ethnicity, national origin, and creed— gender was later added as a protected class)
- 1968 Architectural Barriers Act (Prohibits architectural barriers in federal buildings)
- 1970 Urban Mass Transit Act (Required new purchases of mass transit vehicles be life equipped; APTA sought and won a court injunction barring implementation of the proposed regulations)
- 1973 Rehabilitation Act (Section 504 and related non-discrimination provisions in programs receiving federal funds)
- 1975 Developmental Disabilities Bill of Rights Act (Protection & Advocacy or P&A agencies in each state established)
- 1975 Individuals with Disabilities Education Act (IDEA); Formerly, Education of All Handicapped Children Act (requires appropriate public education for children with disabilities in the least restrictive environment; mainstreaming children with disabilities into regular classrooms)
- 1978 Rehabilitation Act Amendments (Title VII, Comprehensive Services for Independent Living, was created; Part B funded creation and operation of ILCs)
- 1985 Mental Illness Bill of Rights Act (Expanded P&As to cover mental illness)
- 1988 Civil Rights Restoration Act (clarified that any organization or corporation receiving federal funds may not discriminate in any of their programs)
- 1988 Fair Housing Act Amendments (prohibits discrimination against people with disabilities in housing and creates universal design in new construction provisions)
- 1990 Americans with Disabilities Act (creates broad civil rights protections for people with disabilities modeled after the Civil Rights Act of 1964 and Section 504 of the Rehabilitation Act of 1973, including lifts on buses)
- 1999 Olmstead (Supreme Court decision affirmed right to receive services in most integrated setting)
- 2008 ADA Amendment (reaffirmed protections under the ADA to include individuals who can use medication or other devices to mitigate disabilities.)
CENTER FOR DISABILITY RIGHTS – 99 WASHINGTON AVENUE, SUITE 806B – ALBANY, NY 12210
V/TDD (518) 320-7100 – FAX (518) 320-7122 – WWW.ROCHESTERCDR.ORG